
Respiratory system – limiting factor of exercise performance?
In the mention of integrative approach to training and exercise the respiratory system is often a neglected component. The reason for this is partly perhaps breathing has long been ignored and until recently the potential of respiratory muscle training has been hidden. The aim of the blog is therefore to present possible limitations of the respiratory system during exercise and methods used for improving its work.
RESPIRATORY FUNCTION:
Primary function of respiratory system is ventilation, i.e. exchange of gases between the body and the environment. Respiratory system consists of upper and lower airways. When inhaled, the air from the environment first passes through the upper respiratory tract which includes nose, mouth, larynx and throat, and then the lower which includes the trachea, bronchi and the lungs. Air’s journey ends in the pulmonary bubbles called “alveoli” in which changes of gases between the lungs and pulmonary capillaries occur. Upper respiratory tract moisturizes, heats and cleans the small particles from the air. If the inhaled air would not be heated, moisturized and cleaned that would lead to faster drying and narrowing of the airways (bronchoconstriction), sedimentation of harmful particles in them (polluted air, tobacco smoke…), and the creation of frequent inflammatory process.
LIMITATIONS OF RESPIRATORY WORK:
There are groups of athletes who are prone to pulmonary diseases due to spending too much time in potentially harmful training environment. The most common are endurance athletes who train in cold environments and chlorinated swimming pools. (2) Main characteristic of endurance exercise is large total ventilation (> 20 times the normal), which if the air is cold dries up and narrows the respiratory tract, thereby reducing or preventing breathing. The second group of athletes at increased risk are swimmers because they rapidly inhale a large quantity of poisonous by-products of chlorine which are the densest in the air just above the water surface. The result of both mentioned problems is the reduction of air flow to pulmonary alveoli and the decrease of blood saturation with oxygen (hypoxemia) which causes an earlier occurrence of fatigue.
Limitations of the work of the respiratory system could be divided into two categories. One of them are causes than can be willingly changed and the other can’t. The causes on which we generally can’t influence are:
- Disorders of the diffusion of gases between the lungs and capillary. (3)
- Pulmonary shunts. (4)
- Disproportion between ventilation and perfusion (circulation). (4)
Diffusion disorder indicates that the gas diffusion from pulmonary alveoli to their capillaries has been slowed or partially disabled. This may be the case if the inflammatory process in the respiratory system (pneumonia) is present, if the alveoli walls (epithelium) are thick or if liquid has accumulated in the interspace between alveoli and capillaries. (3) At rest, in the first third of the contact between alveoli and capillaries almost all gas exchange occurs. The characteristic of diffusion disorder is a prolonged diffusion time and the inability to maximally oxygenate blood. Diffusion disorders are clinically diagnosed and will not be present in healthy subjects.
The shunt indicates mixing of blood with poor oxygen with oxygen-rich blood. Pulmonary shunts can be anatomic and physiologic. Anatomic shunts are occurring when a blood vessel with deoxygenated blood, that was supposed to pass through the lungs, bypasses the lungs and merges with artery full of oxygen-rich blood. Physiological shunt occurs when the deoxygenated blood passes through a part of the lung that is not ventilated and thus gases between alveoli and capillaries cannot be exchanged. In healthy persons, small shunts are present but they generally will not create a problem at rest and during exercise. (4) The disproportion of ventilation and perfusion occurs when a part of the lung has not been ventilated or when the part of the lung that has been ventilated has no blood flow through the pulmonary capillaries. At rest, for example due to gravity a blood flow through the upper almost 2/3 lungs is low because those are above the heart. Due to a small need for gas exchange during sleep in healthy persons, this phenomenon does not constitute a problem. (5) During exercise the difference in the circulation disappears and then all parts of the lungs are well ventilated and perfused. See Figure 1.
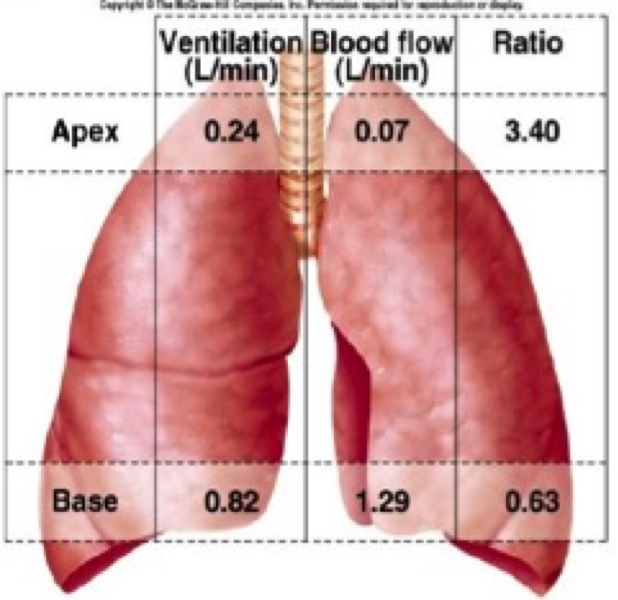
Figure 1. The ratio of ventilation and perfusion in different parts of the lungs at rest. The ratio of ventilation and perfusion in the lower part of the lungs (“Base”) is more favourable than in the upper (“Apex”) due to significantly greater perfusion in the lower part. (Downloaded from:http://slideplayer.com/slide/8379053/26/images/28/Lung+Ventilation/Perfusion+Ratios.jpg)
The second group of causes can be voluntarily influenced. More significant are:
- hypoventilation
- weakness and poor endurance of respiratory muscles
- wrong breathing rhythm
Hypoventilation is reduced pulmonary ventilation. It indicates that the volume of air that enters the lungs at a certain time does not satisfy the needs of the organism and causes hypoxemia. Causes of hypoventilation in healthy persons may be structural disorders of the respiratory tract (e.g.: deviations of the nasal septum) or inadequate frequency and/or volume of breathing. Voluntary breathing control can be positively influenced by correcting a wrongly adopted breathing pattern and get used to some structural deformations. Practical advice to correct the wrong form of breathing is given below.
STRENGTH AND ENDURANCE OF RESPIRATORY MUSCLES:
Inspiratory and expiratory muscles:
Breathing is a process in which a number of muscles are involved. Inhalation is an active process for which it is necessary to consume a greater amount of energy than for the exhalation that is at rest mainly passive process. (7) During training it is necessary to ventilate over 20 times more air and then the exhalation becomes an active process. The amount of energy consumed by the inspiratory muscles at any time is greater than the energy required for work of expiratory muscles. The main inspiratory muscles are diaphragm and external intercostal muscles. During exercise the volume of ventilated air is increased and the accessory inspiratory muscles are activated: Sternocleidomastoideus, Scalenus, levator costarum and serratus posterior superior are included. The main expiratory muscles at rest are internal intercostal, and during the effort are acessory expiratory muscles: transversus abdominis, rectus abdominal, obliqus internus and externus, and serratus posterior inferior. (7) See Figure 2.
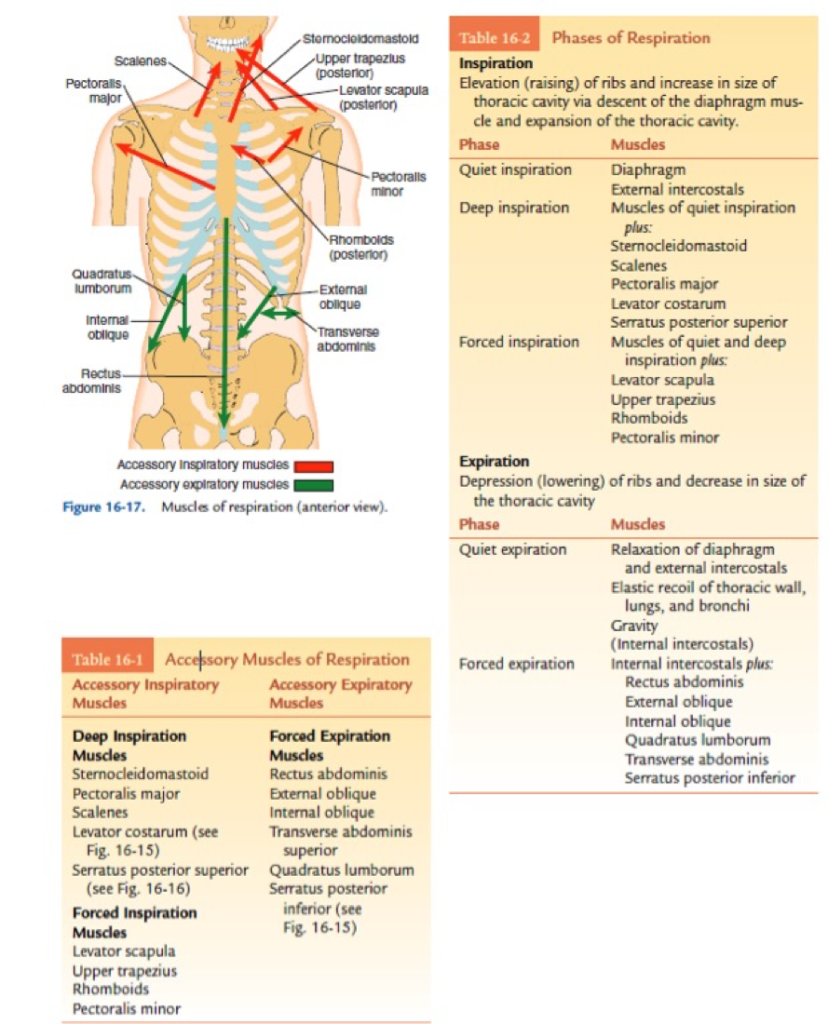
Figure 2. Examination of inspiratory and expiratory muscles. On the left is the anatomical representation of the direction of the force of certain muscles. In the table on the left there is a list of accessory inspiratory and expiratory muscles. In the table on the right there is a list of active muscles in calm and deep inspiration and expiration. (picture is taken from Lynn S. Lippert 2011.) (7)
Breaking the old dogma:
The debate on the function of respiratory muscles was “hot topic” in the 80’s of the previous century. It was then thought that the respiratory system as well as the respiratory muscles could not be a limiting factor of exercise performance.
One argument which defended this assumption says that the respiratory system, irrespective of its training intensity, always has a certain respiratory reserve that it does not use. Respiratory reserve is the difference between the maximum ventilation that can be willingly achieved and the one it achieves in maximal exercise test. It was believed that the respiratory system would use the entire respiratory reserve if the load would require it. Given that body does not use the full capacity during exercise, respiratory system is probably already too developed for the needs of man.
The second argument is related to the diaphragm. It claimed that the diaphragm due to the density of its capillary network is an invincible muscle, and that there is no reason for it to show signs of fatigue, but the limitation to performance should be always sought in peripheral muscle (e.g: quadriceps femoris or pectoralis major or some other muscles).
Despite those bold assumptions, the dogma of the invincibility of the respiratory system and respiratory muscles has been torn down when it was proved that the diaphragm is tiring during exercise. Romer et al., with bilateral stimulation of the frenic nerve have determined that exercise at the intensity of 80-85% VO2 max in duration of 8-10 minutes leads to a decrease in the strength of the diaphragm by 15-30%, which remains present 1-2 hours after the completion of exercise testing. Furthermore, Harms et al. revealed that the emergence of respiratory muscle fatigue reduces blood flow through the extremities because the diaphragm competes with peripheral muscles for blood supply. (9) The mechanism behind the underlying reaction is called respiratory metaboreflex. (10) During high exertion, the body produces large amounts of energy through anaerobic processes, which byproduct is blood lactate. The accumulation of lactate is associated with increase of the aferent discharge over endings of 3 and 4 metabolic fibers in the diaphragm and the increase of the activity of sympathetic nervous system. The increased sympathetic activity will cause vasoconstriction in the skeletal muscles and vasodilation of the blood vessels in the diaphragm, thereby centralizing the bloodstream back to vital organs. (10, 11) See Figure 3
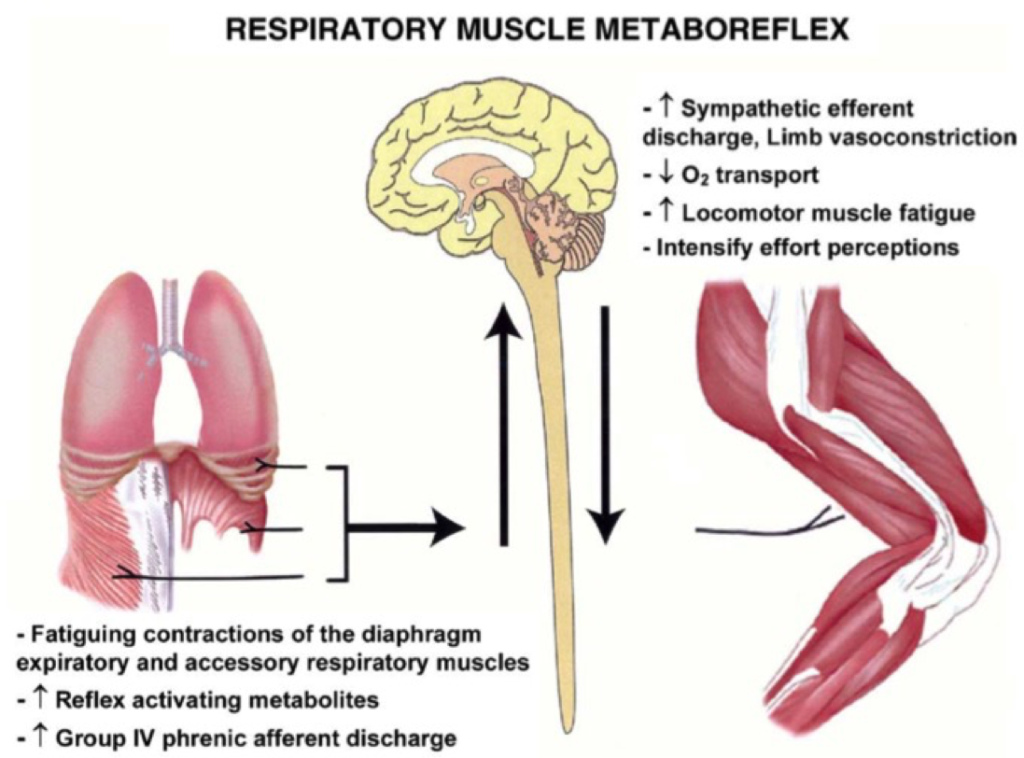
Figure 3. Effects of metaboreflex on the skeletal muscle and diaphragm. (Taken from Dempsey et al. 2006)
By training the respiratory muscles as well as peripheral muscles onset of metaboreflex can be postponed and thereby exercise performance improved. In top athletes, the peripheral skeletal muscles are usually well developed, so the strength and endurance of the respiratory muscles, when it comes to setting records, can be crucial. A minimum period of daily respiratory muscle training that can lead to improved sports performance is 3 weeks.
Practical experiments:
The product of scientific discoveries in the field of respiratory physiology and respiratory muscle training are training models used for improving breathing efficiency. The most frequent type of trainings are strength trainings, breathing pattern trainings during exercise, and the training of breathing with the aim of relaxation. The strength and endurance training of the respiratory muscles are done by performing maximal breaths and/or exhalations with a device that provides resistance during breathing. A more detailed description of the training Protocol and the scientific background of the story can be found in the book “Respiratory Muscle Training: Theory and Practice – Alison McConnell, PhD” and never experimental research/meta analyses. Another way to increase efficiency of breathing is by controlling breathing pattern during exercise. Activities can be cyclical, such as running and cycling, or complex as team sports, various trainings with resistance etc. In cyclical activities it is necessary to synchronise the breathing pattern with the movements of the extremities to make sure that breathing is not chaotic (spontaneous). A concrete recommendation for running is breathing in rhythm 2:2 which indicates that 2 running steps are performed while inhaling and 2 exhaling. At high training intensities frequency and depth of breathing are the most suitable when using that pattern and there is no hypoventilation which would be present in spontaneous breathing or breathing in other forms. If running at relatively lower intensities, other breathing patterns such as 2:3 and spontaneous breathing without a certain rhythm may be applied during light warm-up or jogging. The training of abdominal breathing without external resistance made by external device can’t further improve the strength of the respiratory muscles and consequently the sporting performance in healthy trained athletes. (6) Despite this, such training can be used for relaxation, reduction of stress, improving mental health or as an additional agent in preparation for sports competitions.
Conclusion:
Breathing exercises can be used by everyone regardless of age and health status. The task for coaches and sports practitioners is to apply these findings and make it a standard part of integrative approach to exercise and training.



{kind=link}
{kind=link}
{kind=link}
{kind=link}